crabsallover highlights, key points, comments / links.



 |
| Modified by Chris Street from Guardian Feb 2014 http: //goo.gl/DRAo2R |
'It said that - contrary to decades of public health advice - switching from saturated fats found in foods like butter, cheese and fatty meats, to polyunsaturated fats such as vegetable oils and fish - did not seem to have any benefit for the heart.
This surprised not only me but the people who co-funded the research, the British Heart Foundation (BHF).
Pretty much every respectable health body says that we should cut down on food that is high in saturated fat because it can cause cholesterol levels in the blood to build up.
Raised cholesterol increases your risk of heart disease. Some unsaturated fats can lower blood cholesterol so the assumption has been that this will cut your heart disease risk.
But the analysis of dozens of international studies did not yield clear evidence that switching to mono and polyunsaturated fats reduced the risk of cardiovascular disease. ' says Fergus Walsh. More...
"“Blood test that can predict Alzheimer's,” was the headline used by BBC News, the Daily Mail and The Guardian today. Similar coverage was seen across many of the front pages of other newspapers.
These headlines reflected new research showing how a simple blood test may be able to detect early signs of cognitive decline and mild Alzheimer’s disease.
US researchers discovered a panel of 10 biomarkers that, with 90% accuracy, could distinguish people who would progress to have either mild cognitive impairment or mild Alzheimer’s disease within two to three years, from those who wouldn’t.
While promising, the results were only based on a small group of adults over 70 years old who were studied over five years. Of those who developed mild cognitive impairment or mild Alzheimer’s disease, only 28 people had the test. Consequently, it is not clear if the test has any predictive power in the wider population, is applicable to younger adults, or can predict the disease more than two to three years in advance.
The Daily Mail outlined how, while the research was a breakthrough, experts had warned it would bring “ethical concerns”. This is an important point, because there is currently no cure for Alzheimer’s disease, so some people may prefer not to know they might get it. The current unrefined test means at least one in 10 would be wrongly told they will go on to develop the condition, given the severity of the disease, this may cause significant needless worry."End Quote
How much protein should I eat?
In this study, on average people ate 51% of their calories in the form of carbohydrates, 33% as fat and 16% as protein (11% animal protein). This is likely to be higher in fat and lower in carbohydrates than that recommended on the “Eatwell Plate” which shows the relative proportions of food that we should aim to eat.

"A sensible step that will cut deaths and disability or a mistake that will medicalise millions?
There are starkly opposing views of proposals from the health watchdog the National Institute for health and Clinical Excellence (NICE) to dramatically increase the numbers offered statins.
They are already the most commonly prescribed medicines in the UK, which work by lowering the level of cholesterol in blood. Around seven million people are on the tablets which cost less than 10p a day. It is estimated they prevent around 7,000 deaths a year from heart attacks or strokes. Add to that the tens of thousands of people who are saved from disabling non-fatal attacks and you can see why health experts are keen on statins.
A generation ago cardiovascular disease was common in early middle age. As a result of statins and treatments for reducing blood pressure, the condition has been delayed by around 20 years.
That means two decades more of healthy life for millions of people.
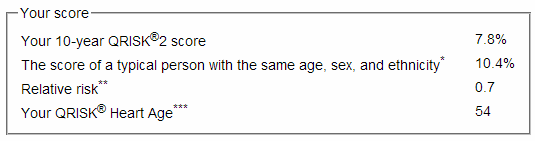
QRISK2
The current guidance from NICE says adults with at least a 20% chance of having a heart attack or stroke in the next 10 years should be offered statins.
That is being lowered to a 10% chance of cardiovascular disease over 10 years.
So how is the risk calculated? You can work out your individual risk by going online to the QRISK2 calculator.
Input factors like your age, sex (men are at greater risk), ethnicity, blood pressure, Body Mass Index, family history, cholesterol level and so on.
It also includes your postcode: heart disease is strongly linked to poverty and deprivation so that will alter your risk too (though clearly you would expect your doctor to take account of your background, rather than just relying on your address).
My risk was well below the 10% trigger for statins. But any smug feeling was quickly despatched when I added a decade to my age.
Once you hit your sixties you can virtually guarantee that your 10-year risk will place you in the statins category no matter how healthy you are.
The effect of the proposals - which have gone out for consultation in England - would be to add millions to the numbers already on statins.
Mark Baker, from NICE, who helped draw up the guidelines said: "You'd probably need to treat about 60 people with statins for 10 years to prevent one heart attack or stroke."
That might not sound like it is worth it, but let's say you treated another six million people, that would prevent 100,000 heart attacks or strokes over a decade.
Diet & exercise
Estimating the health benefits of statins is difficult, and those figures could be an over-estimate. But you can see that - taken over an entire adult population - the potential health benefits are enormous.
So that's the argument in favour. Now the opposite view.
Putting people onto statins is akin to medicalising them for life. Rather than taking a pill to lower cholesterol, the same effect can be achieved through changing their diet and exercise levels.
Even small modifications to lifestyle - taking the stairs or getting off the bus one stop further from your destination - can make positive changes.
Offering sedentary patients a quick fix may simply store up problems for later.
"It's a very bad idea", said Dr Aseem Malhotra a London cardiologist. "Eighty per cent of cardiovascular disease is due to lifestyle and NICE should be concentrating on that aspect rather than offering pills to millions."
Dr Malhotra believes up to one in five people on statins will suffer side effects such as muscle pains, stomach pains or increased risk of diabetes.
NICE says the figure is far lower and serious problems with statins are rare. NHS Choices says "statins are generally well tolerated and most people will not experience any side effects." It lists the range of possible adverse reactions.
Ultimately it will be up to patients to decide, following consultation with their GP. One likely option for many will be to try statins and see whether they trigger any ill-effects.
Statins are saving lives and preventing disability every day. So they are a powerful tool in promoting good health. But people will need to consider carefully before deciding to take a daily pill for decades to come."reposted from: http://www.bbc.co.uk/news/health-26152492
"“Halve sugar intake, say health experts,” The Daily Telegraph reports, while The Guardian tells us that “a can of coke a day is too much sugar”.
The widespread media reports follow new draft international guidelines looking at the healthy maximum recommended levels of sugars in the diet.
Currently, people are advised to have less than 10% of their total energy intake from sugars. However, the new draft guidelines from the World Health Organization (WHO), state that a reduction to below 5% of total energy intake would have “additional benefits”.
An intake of 5% is equivalent to around 25 grams (six teaspoons) of sugar a day for a healthy adult. The WHO’s suggested limits apply to all sugars, including “hidden” sugars added to foods by manufacturers, as well as sugars that are naturally present in fruit juices and honey."